Loneliness is not the same as being alone. We can be alone for hours and feel content; we can be surrounded by family and feel desperately lonely. Loneliness is a feeling — a felt gap between the connection we have and the connection we want.
It is also, increasingly, a public health concern. The World Health Organization has named loneliness a global health priority. National surveys across the UK, the US, and Europe consistently find that significant proportions of the population describe themselves as lonely some or much of the time. And yet, despite how widespread it is, few of us are willing to admit to it publicly. Loneliness carries a particular kind of shame. There is an unspoken cultural assumption that if you are lonely, something is wrong with you — that popular people, well-adjusted people, people who have done the work of building a life, are not lonely. This assumption makes feeling lonely even harder. It implies, quite wrongly, that if you are lonely you are also a loser.
Caregivers of someone with a severe mental illness are particularly vulnerable to loneliness, and that vulnerability takes more than one shape. For some, the relationship with their loved one has consumed so much that other connections have thinned or disappeared — friends drifted away, family kept their distance, the energy for new relationships simply isn’t there. These caregivers may have very few people in their lives at all. For others, the loneliness is different: they are surrounded by people, but those around them cannot or will not take on board what their life is actually like.
This article looks at why caregivers are so vulnerable to loneliness, what it does to a body, and what — given how distinctively difficult their situation is — can be done about it.
What Loneliness Does To The Body
A great deal, as it turns out. The research that has done the most to make this visible is the work of Julianne Holt-Lunstad and her colleagues, who pooled data from hundreds of studies into a meta-analysis. This study found that lonely and socially isolated people show measurably higher rates of early death, with mortality risk increased by roughly a quarter to a third depending on how the comparison is drawn. The popular shorthand — that loneliness is roughly equivalent to smoking fifteen cigarettes a day — comes from this body of work, and while it is rough rather than precise, the underlying claim is broadly true. Loneliness, sustained over time, shortens lives at a scale comparable to major medical risk factors such as smoking.
A separate meta-analysis published in the journal Heart found similar results for heart health specifically. Poor social relationships are associated with around a 29% increased risk of coronary heart disease and a 32% increased risk of stroke.
So why does loneliness have such a profound and harmful effect on the body? The human nervous system evolved expecting connection — we only survived as a species because we lived in groups. It therefore registers the absence of connection as a major threat or stressor.
The problem is that we have nervous systems that are designed to be stressed for a short time — running away from an animal that wants to eat us — and then quickly return to a non-stressed state. The stress response drives inflammation which in the short term is good: it would help us heal from a wound received when running away from that pesky animal. But being stressed for long periods creates low-grade, persistent inflammation. And it is this chronic inflammation — not loneliness directly — that increases susceptibility to a wide range of diseases. Cardiovascular disease, type 2 diabetes, autoimmune conditions, dementia, depression: these have all been linked to inflammation. Loneliness is not, in any simple sense, causing these conditions. It causes changes in the body that make these conditions more likely.
What This Looks Like In Caregivers
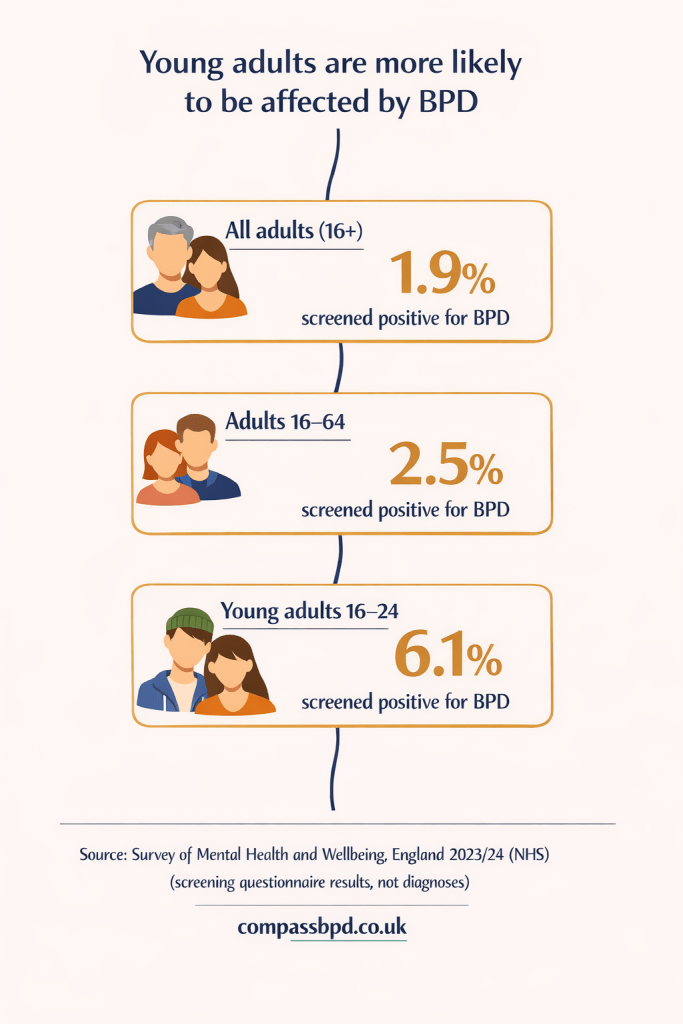
We don’t yet have research specifically on loneliness in BPD caregivers. However, a 2014 study found that caregiving in this group caused high levels of grief and burden — even higher than in those caring for loved ones with other mental illnesses, such as schizophrenia.
And a 2023 review identified stigma as a distinctive cause of caregiver isolation. The cultural shame around having a loved one with mental illness, especially one as poorly understood and as poorly portrayed as BPD, pushes caregivers away from the very people who might otherwise be there for them. They keep the diagnosis private, edit what they tell friends, sidestep the questions they cannot answer truthfully.
Why The Standard Advice Doesn’t Quite Fit
The standard loneliness advice, when it appears in articles and self-help books, almost always points outward. Connect more. Disclose more. Get out more. Build your support network. For many people in many situations, this is reasonable advice. If you are caring for someone with BPD, it can be more complicated.
Disclosure to other people — friends, extended family, colleagues — does not always produce the positive effect the advice assumes it will. Instead it may produce well-meaning but unhelpful responses: you really need to put yourself first, or have you thought about leaving? Or a hasty change of subject because the situation is too uncomfortable to sit with. And your loved one with BPD is not always the person you can turn to for this. Their dysregulation can crowd out the bandwidth for anyone else’s experience — and in some relationships, such as parent and child, it would not be right to turn to them anyway.
The danger is that you try the standard advice, find it does not reliably help, and conclude that the loneliness is your own failure — that you must be doing something wrong, or that you are somehow defective at human connection. You are not. The standard advice works less well for you not because you are failing at it, but because it assumes that the people you disclose to will be able to validate what you’re going through. And this isn’t what often happens in real life. Many of us just aren’t very good at the skill of validation. There are a lot of reasons for this — enough to write another article. Suffice to say here that the odds are you are just as likely — perhaps even more so — to be offered advice, solutions, or to be dismissed, if you open up about your experience of being a caregiver to someone with BPD.
Tackling It From A Different Angle
The thing about a problem you cannot easily solve head on is that you can sometimes tackle it sideways instead. Two side approaches are worth knowing about, both supported by good research. And you don’t need to pick and choose, they can work alongside each other.
The first is purpose. A study published in 2015 tested whether any psychological factor produced the opposite pattern to loneliness in the body. They found that a sense of purpose and meaning in life was associated with a reversal of the inflammatory pattern. The size of the protective effect was roughly equal to the size of loneliness’s harmful effect.
What is great about this is that purpose is something you can be in control of. It’s personal. It doesn’t come from other people — it comes from inside. It can be located in the action of caregiving itself, or in something else entirely — a piece of work, a creative project, a community role, a private commitment to a cause. The biological benefits do not depend on the source. What they require is a relationship, sustained over time, between you and something you find meaningful.
The second side approach is the arts. This is the work of Professor Daisy Fancourt. Her recent book Art Cure (2026) gathers the evidence: regular engagement with the arts is associated with reductions in inflammatory markers, lower stress hormone levels, better cardiovascular function, and, at the population level, reduced mortality.
The research distinguishes between two ways of engaging. Participatory engagement — singing, dancing, drawing, playing an instrument, writing, joining a choir or a community group — can produce measurable benefits. Receptive engagement — listening to music, reading, going to a museum, watching a film, looking at art — can also produce benefits, albeit not quite so strong. The distinction matters because it widens the door considerably. If you have no time for a weekly choir, you can still sit down and listen to music at home. If you cannot afford theatre tickets, you can still take a library book to bed. None of this needs to be performed for anyone. None of it requires talent. The point is the engagement, not the production.
So the things you might already do for relief — putting on music when the house is quiet, reading a novel before sleep, sketching for half an hour on a Saturday morning — are not indulgences. They can change your biology for the good. They can potentially reduce the inflammation that loneliness drives up.
When You Have More Than One Source Of Resilience
When you have several different sources of resilience — purpose somewhere in your life, regular contact with the arts, perhaps physical movement, perhaps a faith, perhaps a single trusted friend — you become less dependent on any one of them in particular.
If you have built some inner resources, you don’t need your friend to respond to you ‘perfectly’ when you have a catch-up to feel better. The process of getting it off your chest might be enough, because it is not being asked to do all the work of relieving your distress.
This is not an argument against connection. Where genuine connection is available — be that from a friend, a therapist, a peer in a support group — it can be incredibly valuable. The point is more modest: if you have found that the standard advice on how to tackle loneliness doesn’t quite work for you, you are not without options. There are alternatives out there, and evidence that they can help.
Conclusions
We need to be realistic. Loneliness has structural causes that no amount of personal practice can resolve. The stigma around BPD is unlikely to disappear any time soon. The wider challenges of caregiving — its invisibility, its open-endedness — are not changed by someone writing, listening to music, or finding purpose. And in your own life, the people around you may continue to struggle to take on board what you’re living through.
However you are not without resources, even when you are without witnesses. The body’s response to loneliness is inflammation. Inflammation can be reduced. And on the days when you do open up to someone and feel truly seen, who knows? Maybe the effects will be all the stronger, because of all the work you have done to build a body that can receive the relief it offers.
Sources And Further Reading
Holt-Lunstad, J., Smith, T. B. & Layton, J. B. (2010). Social Relationships and Mortality Risk: A Meta-analytic Review. PLoS Medicine, 7(7), e1000316.
Valtorta, N. K., Kanaan, M., Gilbody, S., Ronzi, S. & Hanratty, B. (2016). Loneliness and social isolation as risk factors for coronary heart disease and stroke: systematic review and meta-analysis of longitudinal observational studies. Heart, 102(13), 1009–1016.
Bailey, R. C. & Grenyer, B. F. S. (2014). Supporting a person with personality disorder: A study of carer burden and well-being. Journal of Personality Disorders, 28(6), 796–809.
Guan, Z., Poon, A. W. C. & Zwi, A. (2023). Social isolation and loneliness in family caregivers of people with severe mental illness: A scoping review. American Journal of Community Psychology, 72(3–4), 443–463.
Cole, S. W., Levine, M. E., Arevalo, J. M. G., Ma, J., Weir, D. R. & Crimmins, E. M. (2015). Loneliness, eudaimonia, and the human conserved transcriptional response to adversity. Psychoneuroendocrinology, 62, 11–17.
Fancourt, D. (2026). Art Cure: The Science of How the Arts Transform Our Health. Cornerstone Press.