In this article I talk about crisis, but I don’t necessarily mean a medical emergency. I mean any episode of extreme emotional intensity and dysregulation. In the aftermath of a loved one’s crisis, many caregivers instinctively replay what happened — what was said, what was done, what they should have said instead — to make sense of their distress. But mental replay provides only part of the picture. The body was there too, experiencing all of it, and my theory is that understanding what happens at the body level could be the key to recovery.
What the Research Tells Us
There hasn’t been a great deal of research into the physical and mental impact on caregivers who have a loved one with BPD, but what has been done shows that the impact can be profound.
A systematic review by Bailey & Grenyer (2013), published in the Harvard Review of Psychiatry, found that caregivers of people with BPD experience higher levels of burden and grief than caregivers of other serious mental illnesses, including schizophrenia.
Their follow-up study (2014) found that BPD caregivers reported symptoms at levels consistent with mood disorders, anxiety, and PTSD.
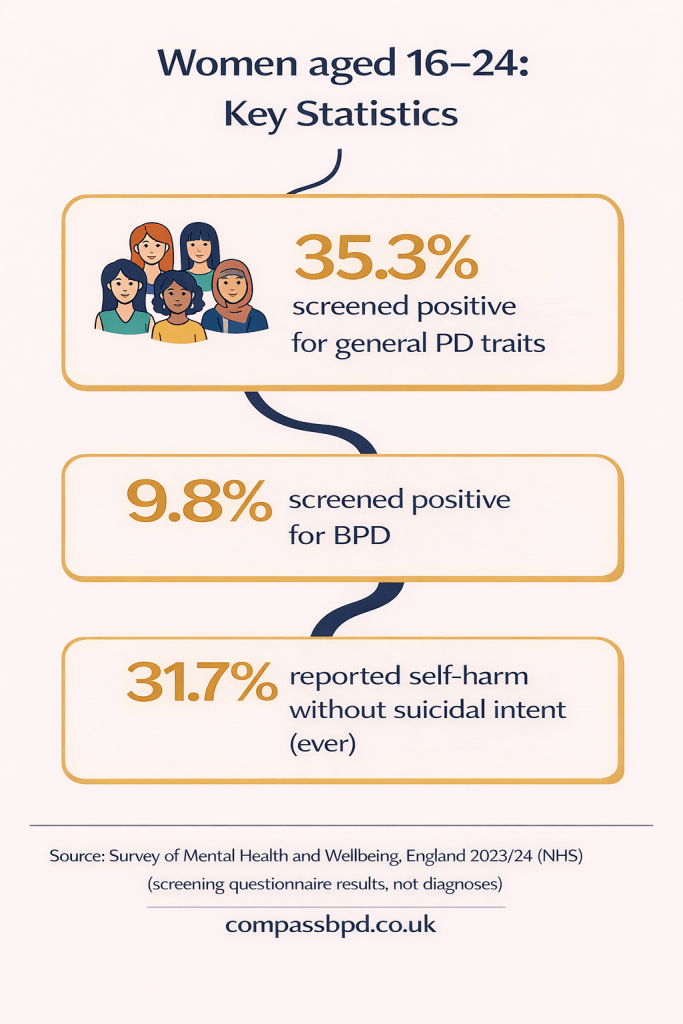
More recently, a 2025 study (Tempia Valenta et al.) noted significant psychological and somatic distress in BPD caregivers — physical symptoms caused or worsened by chronic stress, such as headaches, stomach problems, and sleep disruption.
I haven’t found research that explores why caregivers experience this level of physical and psychological impact. What follows is my attempt to provide one answer to that question — drawing on established science around the body’s stress response and applying it specifically to the experience of caring for someone with BPD.
Your Body Has a Plan
When your brain perceives a threat — whether a physical danger or your loved one in crisis — it triggers a cascade of changes designed to keep you alive. Adrenaline surges, your heart rate climbs, muscles tense, breathing quickens. Cortisol follows, keeping you alert and mobilising energy. Blood flow redirects away from both digestion and your “thinking brain” toward the systems that help you survive.
This is the fight-or-flight response. It evolved to handle physical threats requiring immediate action. The stress hormones flood your system, you fight or run, and the exertion uses up that mobilised energy. Then your parasympathetic nervous system kicks in to restore calm. Threat over. Cycle complete. System resets.
The key word is “complete.” The stress response has a beginning, middle, and end — and researchers like Peter Levine have argued that physical action is what closes the loop, the body’s way of saying: the danger has passed, stand down.
What Happens When the Cycle Can’t Complete
When your loved one with BPD is highly dysregulated, or in crisis, your body can experience this as a threat. It then mobilises exactly as it’s designed to, but the context of caregiving — the love, the responsibility, the need to stay in relationship — means the stress cycle may never complete. And this is true regardless of how you respond:
- Holding everything in. You stay calm on the surface while your nervous system screams underneath. The energy mobilised for action has nowhere to go — it stays in the muscles, the clenched jaw, the tight shoulders, the buzzing restlessness that lingers long after the crisis is over.
- Fighting back. You shout, argue, match the intensity. It looks like stress is being discharged, but what often follows is guilt and self-recrimination — one incomplete cycle giving way to another.
- Walking out. You leave the room, drive away. This comes closest to completing the flight response, but worry, guilt, and hypervigilance about what you’ll return to can keep your nervous system activated even though you’ve physically moved away.
- Shutting down. You go numb, feel detached, experience a strange flatness. This is the freeze response — the nervous system’s last resort when neither fight nor flight seems possible. It can be the hardest state to recognise as stress, because it doesn’t feel like agitation. It feels like nothing.
- Fawning. You pour all that activated energy into appeasing and accommodating, doing whatever it takes to de-escalate. Outwardly calm, but underneath the nervous system is working overtime.
There are also approaches that can help people with BPD and their loved ones respond more skilfully in times of crisis, in ways that reduce stress on both sides — and future articles will explore these. But even with better tools, the fundamental challenge remains: your body is likely activating a survival response in a situation where survival instincts aren’t always what’s needed.
Whatever your response looks like, it’s the situation itself — not a personal failing — that makes the stress cycle so hard to complete.
What “Stuck Stress” Feels Like
When a stress cycle doesn’t complete, the after-effects show up in the body in one of two ways:
Agitation: a restless, buzzing energy that won’t settle. Your body is still primed for action that never happened — the energy sitting in your muscles, waiting to complete a response that got interrupted.
Crash: a heavy, flu-like exhaustion that descends hours or sometimes days after a crisis. Your body went through a significant physical event, even though from the outside it might have looked like you were just standing in your kitchen.
Neither is a sign of weakness. Both are signs of a body that has been through something real and hasn’t yet completed its natural recovery.
Over time, when these cycles repeat without resolution, the effects can become chronic — persistent headaches, stomach problems, disrupted sleep, unexplained aches. I believe this may be the mechanism behind the somatic distress that research is now documenting in BPD caregivers.
Why the Standard Advice Sometimes Misses the Mark
If you’ve been told to try yoga, take a bath, go for a walk, or practise deep breathing — and sometimes it helps and sometimes it doesn’t — there are good reasons for that.
If your body mobilised for a sprint, a gentle stroll doesn’t match the energy that was prepared. When your system is highly activated, stillness can feel like being trapped rather than calm. And when your nervous system is dysregulated, your thinking brain goes partially offline — so strategies that rely on reasoning your way through it may not reach the part of you that needs them.
These techniques aren’t useless — but they’re not always the right tools for the moment.
Why This Matters
Understanding the stress cycle answers a question many caregivers ask: my loved one is the one suffering, not me — so why do I feel physically and mentally dreadful? Because your body has been through something real, repeatedly, and it deserves help completing its natural recovery.
Where This Takes Us Next
If stress gets stuck because the cycle can’t complete, the obvious question is: what helps it complete? There’s a growing body of research offering practical answers — and future articles in this series will explore them.
Sources and Further Reading
Bailey, R. C. & Grenyer, B. F. S. (2013). Burden and support needs of carers of persons with borderline personality disorder: A systematic review. Harvard Review of Psychiatry, 21(5), 248–258.
Bailey, R. C. & Grenyer, B. F. S. (2014). Supporting a person with personality disorder: A study of carer burden and well-being. Journal of Personality Disorders, 28(6), 796–809.
Tempia Valenta, S. et al. (2025). Psychoeducation for caregivers of individuals with borderline personality disorder: A randomized controlled trial of multiple family group therapy. Personality and Mental Health.
Levine, P. A. (1997). Waking the Tiger: Healing Trauma. North Atlantic Books.
Porges, S. W. (2011). The Polyvagal Theory. Norton.
Payne, P., Levine, P. A. & Crane-Godreau, M. A. (2015). Somatic experiencing: using interoception and proprioception as core elements of trauma therapy. Frontiers in Psychology.
Gerritsen, R. J. S. & Band, G. P. H. (2018). Breath of Life: The Respiratory Vagal Stimulation Model of Contemplative Activity. Frontiers in Human Neuroscience.
NEABPD (2025). Managing Suicidality & Trauma Recovery (MSTR): A Course for Parents in Distress.